|
| wikipedia.org |
An incredible amount of data on global mortality and morbidity is now available for free from
The Lancet online. These data are from the
Global Burden of Disease Study (GBD), a herculean effort sponsored by the
Bill & Melinda Gates Foundation.
These data have already generated a significant amount of press (see a nice article in The Washington Post
here); this project is simply amazing.
I have to admit I felt like a kid on Christmas morning when I first started going through these articles... there are few things epidemiologists like more than
data. And there are a whole lot of data associated with the GBD project.
Here are some things I found notable; my comments mainly focus on Latin America as our
medical/ public health project is in Honduras. There is a
whole lot more in these data than my comments below reflect so I encourage you to take a look at these articles-they are
all available free online.
Deaths due to communicable, neonatal, maternal and nutritional causes dropped from 15.9 million in 1990 to 13.2 million in 2010, a 17% decrease. In contrast, deaths due to non-communicable disease increased by a little under 8 million, accounting for approximately 66% of all deaths.
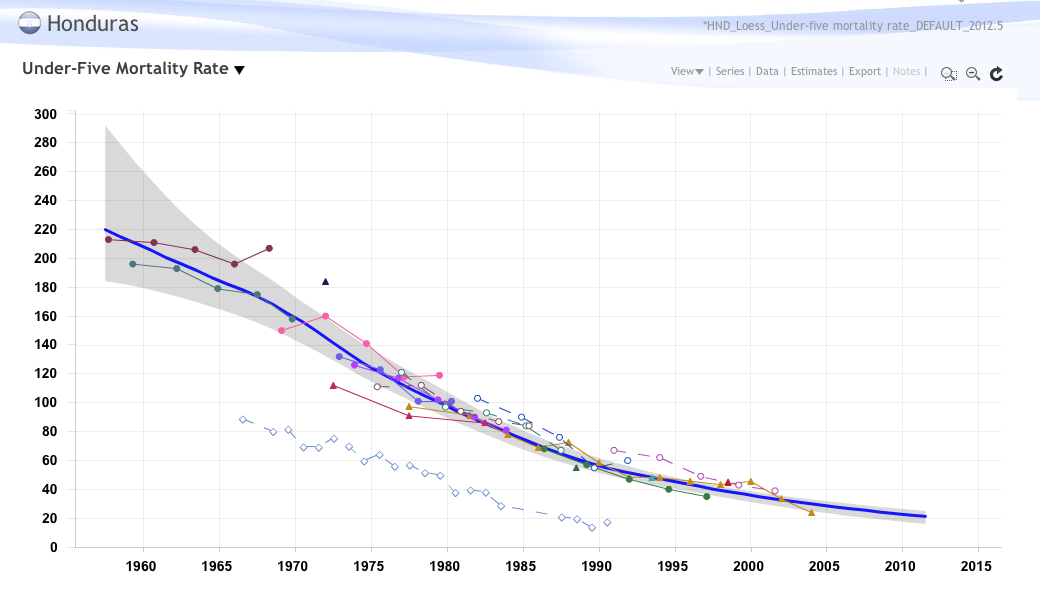
Deaths in children less than 5 years of age dropped a whopping 59% since 1970 (from 16.4 million in 1970 to 6.8 million in 2010).
The male/ female life expectancy in Honduras has gone up from 54.7/ 58.6 in 1970 to 70.5/ 73.2 in 2010. In contrast, the male/ female life expectancy in the US in 1970 was 67/ 74.6 and 75.9/ 80.5 in 2010. There is still a marked discrepancy between 'developed' and 'developing' nations, but significant gains have been made; there are regional and country-specific differences, of course, but overall people are living longer.
The global burden of disease has shifted away from premature deaths and from deaths due to communicable diseases to deaths caused by non-communicable diseases. The top three diseases in terms of disability-adjusted life years ("DALYs") in 1990 were: 1) lower respiratory infections, 2) diarrhea and 3) preterm birth complications. In 2010 these had dropped to #2, #4 and #8, respectively. In 2010 ischemic heart disease was #1 (up from #4 in 1990) and stroke was at #3 (up from #5 in 1990). In terms of DALYs, HIV/AIDS went up dramatically between 1990 to 2010: from #33 to #5.
There were significant regional differences in DALYs attributed to various disease states. For instance, in central Latin America interpersonal violence was the #1 contributor to DALYs, with ischemic heart disease ranking #2. In contrast, in the region including the US interpersonal violence was the 25th highest contributor to DALYs.
Looking across 67 risk factors for 21 world regions there was an overall shift in global disease burden/ morbidity from risk factors promoting childhood communicable diseases to those promoting adult, non-communicable diseases.
In 2010 the biggest DALY risk factors were high blood pressure, tobacco smoking and alcohol use; in most of Latin America the greatest risk factor was alcohol use. Back in 1990 the greatest DALY risk factors were childhood underweight and indoor air pollution from solid fuel use.
These Global Burden of Disease data are absolutely fantastic and provide a comprehensive, methodologically sound global picture of the leading causes of morbidity and mortality and how these have changed over the past twenty years; more importantly, these data can be looked at by country and region. This information should be used by the public health and development communities to target interventions that will have the greatest impact for a given country/ region.
From an overall disease burden perspective, the world is becoming a different place than it was twenty years ago. Our health systems need to adjust to account for a growing population of older people with significant comorbidities such as heart disease, diabetes and osteoarthritis. This is true for both developed and developing countries.